A new report has revealed substantial variation in the hourly earnings of Australian medical specialists and it isn’t entirely clear what’s justifying it.
The ANZ Melbourne Institute’s Health Trends – Specialists report says greater fee transparency is needed as part of the wider policy challenge of ensuring that we are realising full value from the country’s growing health expenditure.
And insurers and professional member bodies are likely best placed to drive greater transparency in the sector, says study leader Professor Anthony Scott.
“In the current market, patients have little or no information at the point of referral and, therefore, cannot make informed choices regarding the value proposition of different providers and treatments,” says Professor Scott, Program Director Health Economics at the University of Melbourne’s Melbourne Institute of Applied Economic and Social Research.
“Whether fee transparency will lead to a reduction in fee variation and eradicate some of the very high fees causing understandable public concern, will really depend on how GPs and patients access the information at the time of referral and how specialists themselves react.”
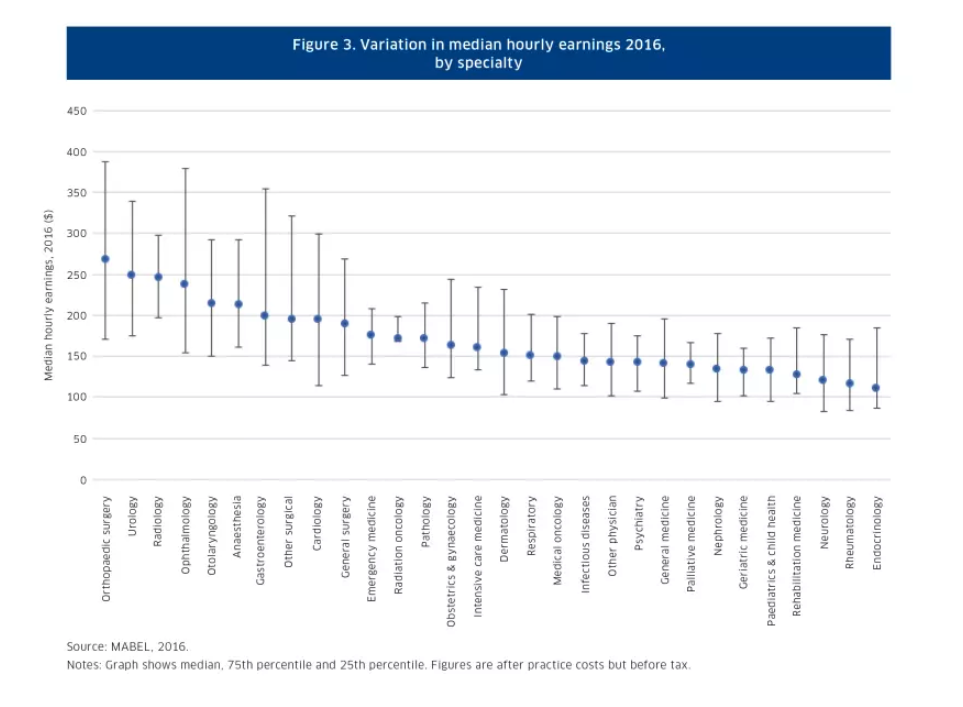
The report cites Professor Scott’s Medicine in Australia: Balancing Employment and Life survey of doctors that found significant within-specialty and between-specialty variation in earnings, particularly between surgical and non-procedural specialty groups.
The highest earning group is orthopaedic surgeons, where median hourly earnings are 2.4 times higher than those of endocrinologists at the lowest end of the scale. But among orthopaedic surgeons themselves, hourly earnings at the top are 2.3 times those at the bottom.
Medicare data also shows significant fee variation within-specialty. For example, in 2016 within neurology there was a 125 per cent difference between consultation fees at the lowest and highest ends of the scale.
Health spending driven by volume not fee rises
But on the positive side, the report found that rising spending in health is being driven by volume, not fees. Average prices per service, including both the government’s Medicare fee and the provider fee, actually fell in real terms by 0.15 per cent in the ten years to 2015-16.
Research suggests some of the fee disparity reflects private practice costs, location, equipment, the time required and the complexity of procedures. But Professor Scott says these cost inputs aren’t the full story.
While a provider’s reputation and expertise could also be expected to drive fees, he says the problem is that customers (both patients and general practitioners) generally lack the information to make these judgements.
“The fact that GPs and patients have little information on quality and costs suggests that other factors are likely playing a role,” says Professor Scott.